Tumor-Infiltrating Lymphocyte Therapy for Advanced Melanoma: Ready for Prime Time?
2023
Melanoma
In this Perspectives on the Science piece, published in the Journal of Cutaneous Oncology, we reflect on the impact of the recently published article “Tumor-Infiltrating Lymphocyte Therapy or Ipilimumab in Advanced Melanoma”.
Emily Y Kim 
Sophia Z. Shalhout
Howard L. Kaufman
Kevin S. Emerick
Vishal A. Patel
Isaac Brownell
David M. Miller
Keywords
Melanoma, Tumor-Infiltrating Lymphocytes
Featured Article
Tumor-Infiltrating Lymphocyte Therapy or Ipilimumab in Advanced Melanoma. Rohaan et al. NEJM. 2022 Dec 8;387(23):2113-2125.
Introduction
On January 9th, 2023, the multi-institutional Cutaneous Oncology Interest Group Journal Club reviewed the recently published NEJM article “Tumor-Infiltrating Lymphocyte Therapy or Ipilimumab in Advanced Melanoma”(Rohaan et al. 2022). Participants included clinicians and investigators from Massachusetts General Hospital, Mass Eye and Ear, Brigham and Women’s Hospital, the National Institutes of Health, George Washington Medical Center, the University of Pittsburgh Medical Center and the Northwestern Feinberg School of Medicine. Importantly, the comments in this article represent the views of the authors of this Perspectives on the Science piece after the Journal Club. It does not represent views of any other members of the Interest Group or the affiliated institutions. In this article we provide a summary of the discussion regarding this important contribution to the literature.
Background for the Study
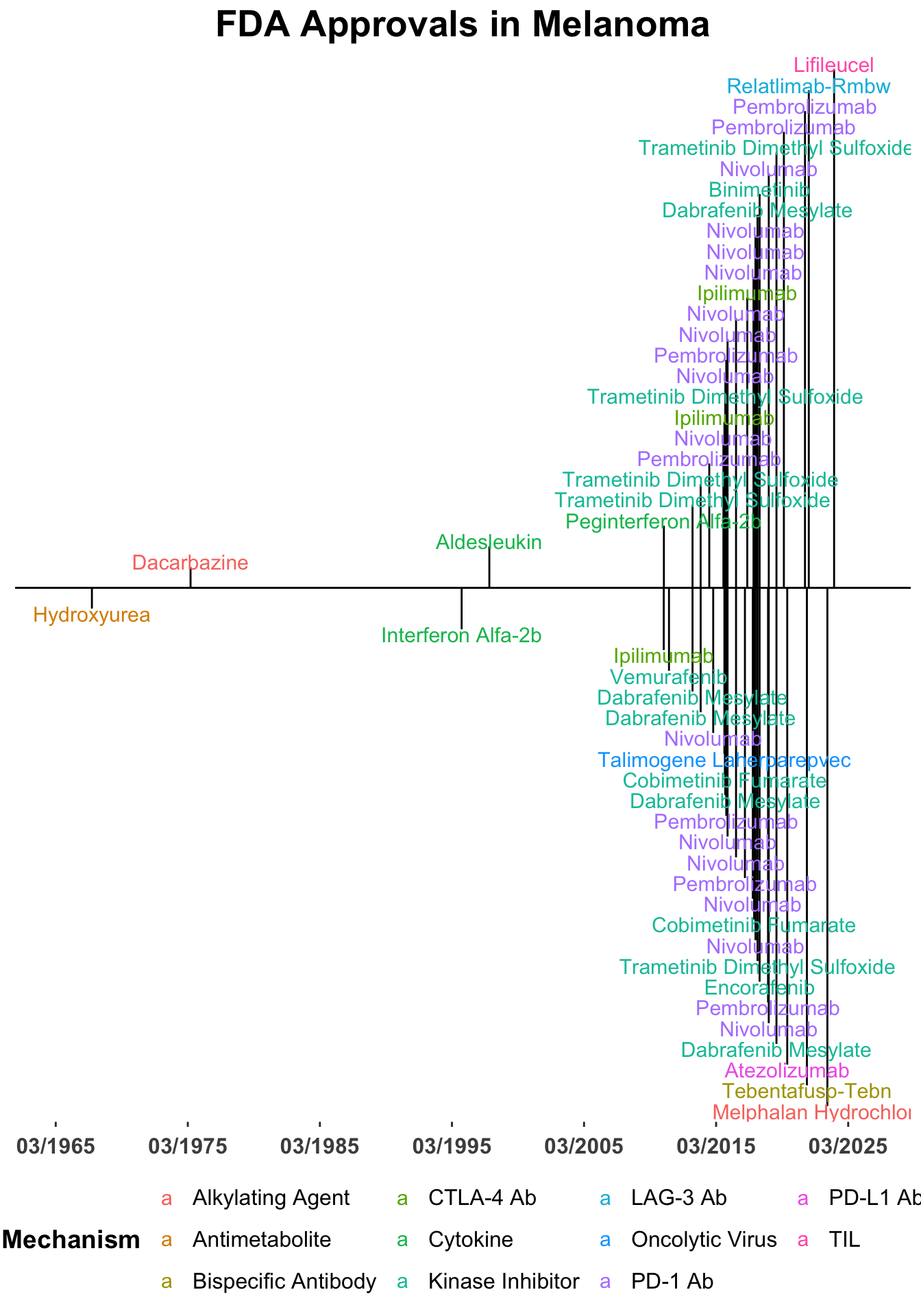
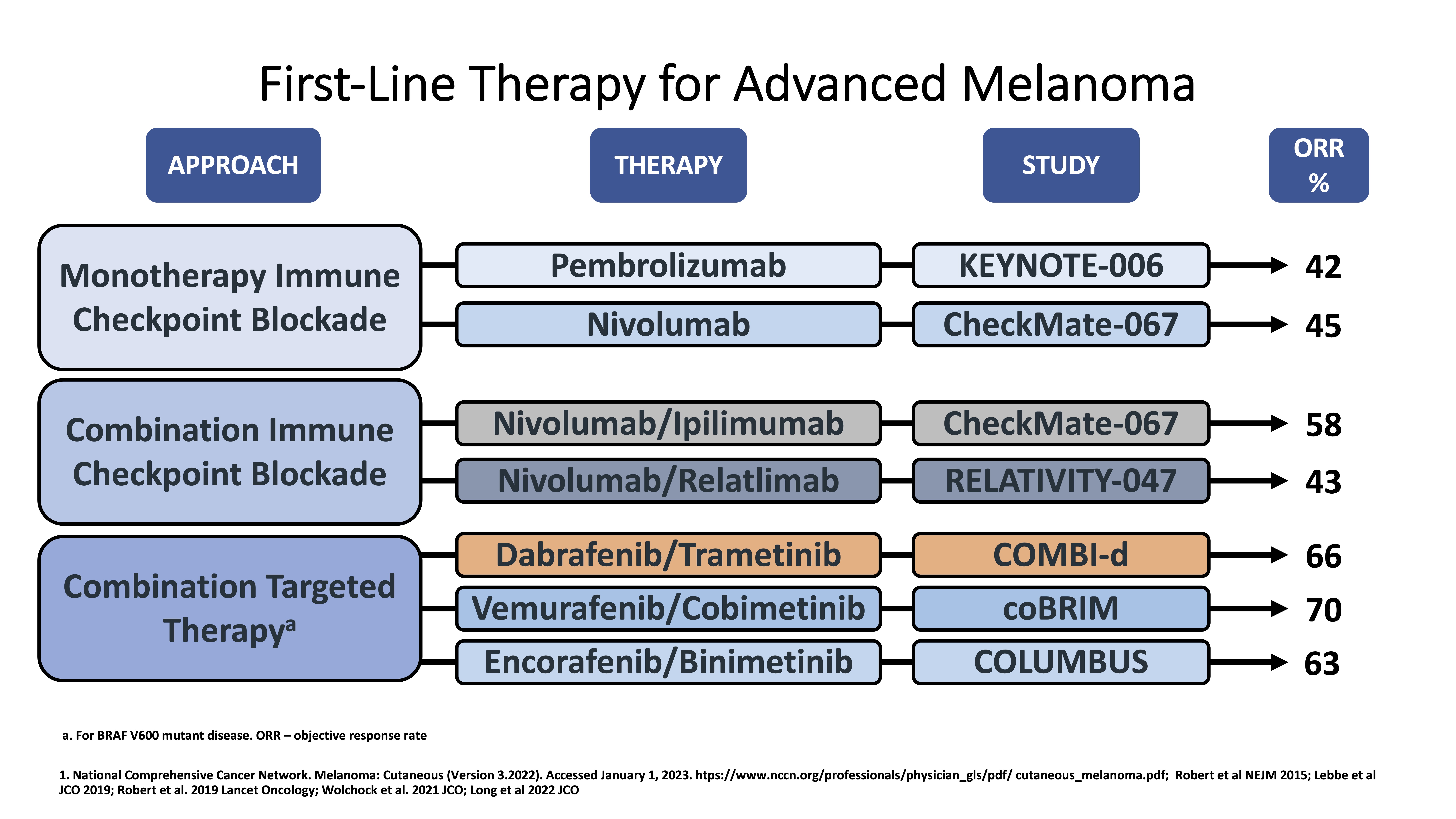
Treatment options for melanoma have advanced greatly in the last several years and continue to evolve (Figure 1). Landmark studies such as KEYNOTE-001/006 and CheckMate-066 have led to single-agent immunotherapy with anti-PD-1 immune checkpoint inhibitors becoming a first-line treatment options for advanced, unresectable melanoma (Figure 2)(Hamid et al. 2019; Robert et al. 2015; Robert, Ribas, et al. 2019; Schachter et al. 2017; Petrella et al. 2017). Subsequent studies such as CheckMate-067 and RELATIVITY-047 have positioned dual immune checkpoint blockade (ICB) with aPD-1/aCTLA-4 and aPD-1/aLAG-3 monoclonal antibodies as additional options in the front-line setting for appropriate patients (Wolchok et al. 2017; Tawbi et al. 2022; Long et al. 2022). In addition combined BRAF and MEK inhibition is an option for melanomas with BRAF mutations (Robert, Grob, et al. 2019; Dummer et al. 2018).
Figure 2. Front-line therapy in advanced melanoma.
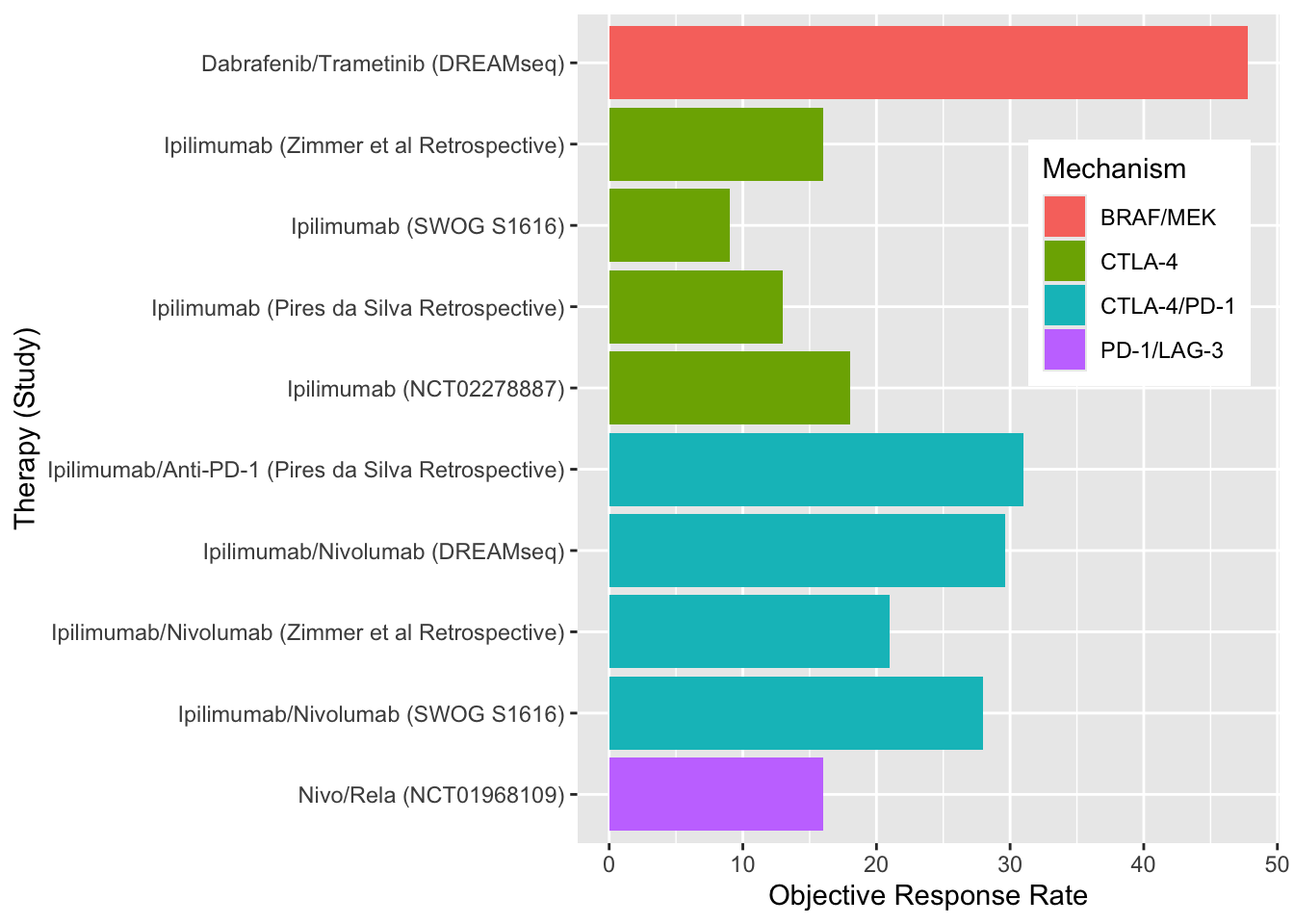
Despite these treatment measures, primary and acquired resistance is common for all front-line therapeutic options. Unfortunately, outcomes with ICI and targeted therapies in the second-line setting have been disappointing (Figure 3). (Atkins et al. 2023; Pires da Silva et al. 2021) Subsequently, the 5 year mortality rate in patients with stage IV disease is 50%.
Figure 3. Efficacy of second-line therapy in advanced melanoma.
Adoptive cell therapy with tumor-infiltrating lymphocytes (TILs) has shown clinical utility in melanoma since the 1990s (S. A. Rosenberg et al. 1994). In this process, tumor-resident T cells from a patient’s tumor are extracted and expanded ex-vivo. The patient is administered preparative lymphodepleting chemotherapy, often with cyclophosphamide and fludarabine, before the T-cells are infused back into the patient with interleukin-2 to further enhance in vivo expansion of cells and boost the antitumor response. While results have varied, multiple phase I and II trials have shown response rates around 50% (Berg et al. 2020; M. E. Dudley et al. 2008; Steven A. Rosenberg et al. 2011; Besser et al. 2010; Ellebaek et al. 2012; Andersen et al. 2016; M. Dudley et al. 2022; Pilon-Thomas et al. 2012). Several of these studies are summarized in Table 1. C-144-01, a recently reported study of LN-144 TIL therapy in patients who failed anti-PD-1 immunotherapy reported an objective response rate of 31.4% in a pooled analysis of consecutive cohorts, highlighting potential utility of TIL therapy for patients who have had disease progression on first-line options (Sarnaik et al. 2021).
Study Design
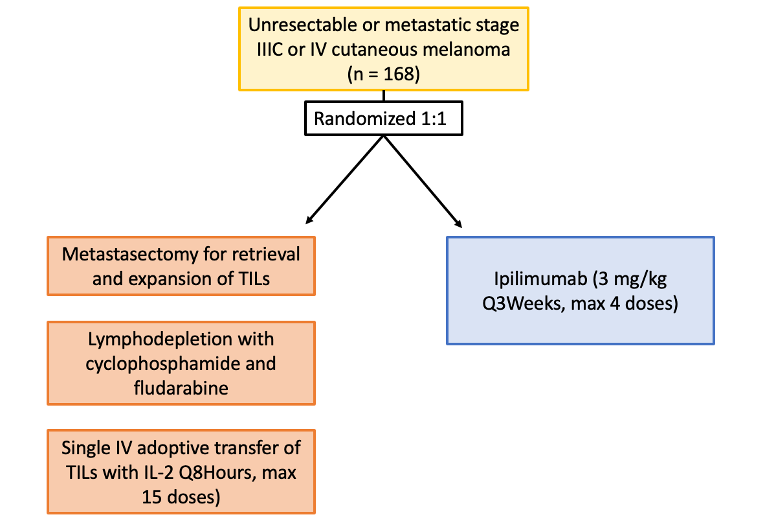
The study by Rohaan et al. was a phase III, multicenter, open-label trial including Dutch patients age 18-75 with unresectable stage IIIC or IV melanoma. Patients were randomized in a 1:1 ratio to receive TIL or anti-cytotoxic T-lymphocyte antigen 4 (CTLA4) therapy (ipilimumab) (Figure 4). Patients assigned to the TIL group underwent a metastasectomy for retrieval and expansion of TILs, then received nonmyeloablative, lymphodepleting chemotherapy with cyclophosphamide and fludarabine. Single intravenous adoptive transfer of TILs was followed by high-dose interleukin-2 every 8 hours, for a maximum of 15 doses. Patients in the ipilimumab group received 3 mg per kilogram of body weight every 3 weeks, for up to 4 doses. The primary end point was progression-free survival, defined as the time from randomization to first disease progression or death. Secondary endpoints included progression-free survival (PFS), objective response, complete response, overall survival, health-related quality of life, and safety.
Figure 4. Study design.
Main Findings
168 patients (86% with disease refractory to anti–programmed death 1 treatment) were assigned to receive TILs (84 patients) or ipilimumab (84 patients). Median PFS in the TIL group was 7.2 months, significantly longer than 3.1 months in the ipilimumab group. Objective response rates were 49% in TIL group and 21% (95% CI, 13 to 32) of patients in ipilimumab group. 20% of patients in the TIL group achieved complete response, compared to 7% in the ipilimumab group. At the time of the data cutoff, the overall median follow-up was 33.0 months. Median overall survival was 25.8 months in the TIL group and 18.9 months in the ipilimumab group. In regards to safety, treatment related adverse events occurred in all patients in the TIL group and in 96% of those in the ipilimumab group. All patients in the TIL group experienced grade 3 adverse events, largely due to chemotherapy-related myelosuppression, while 57% of patients in the ipilimumab group experienced grade 3 or higher adverse events. Overall, patients in the TIL group had higher mean health-related quality of life scores than those in the ipilimumab group, though scores varied for different symptoms.
Discussion Points
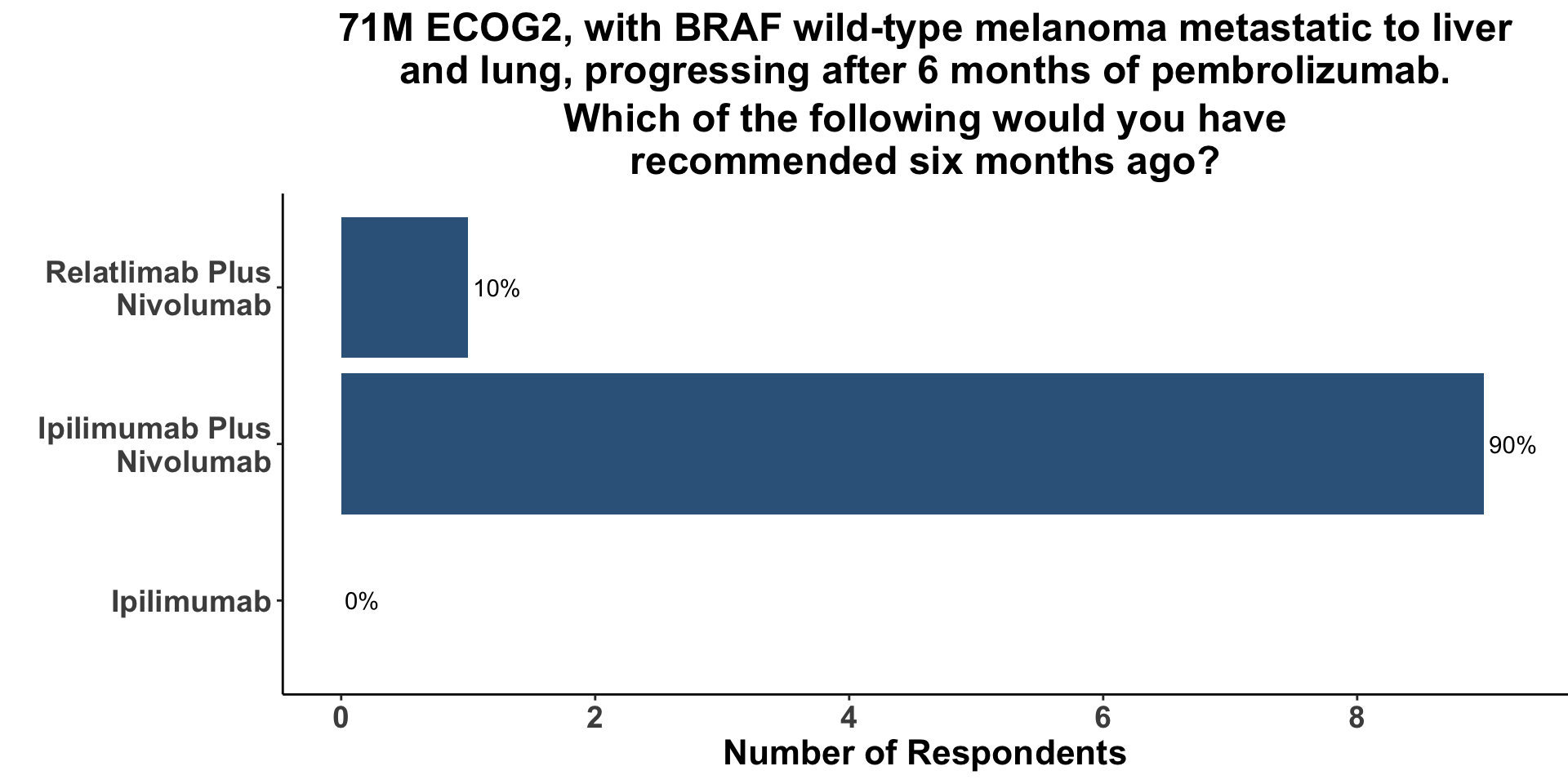
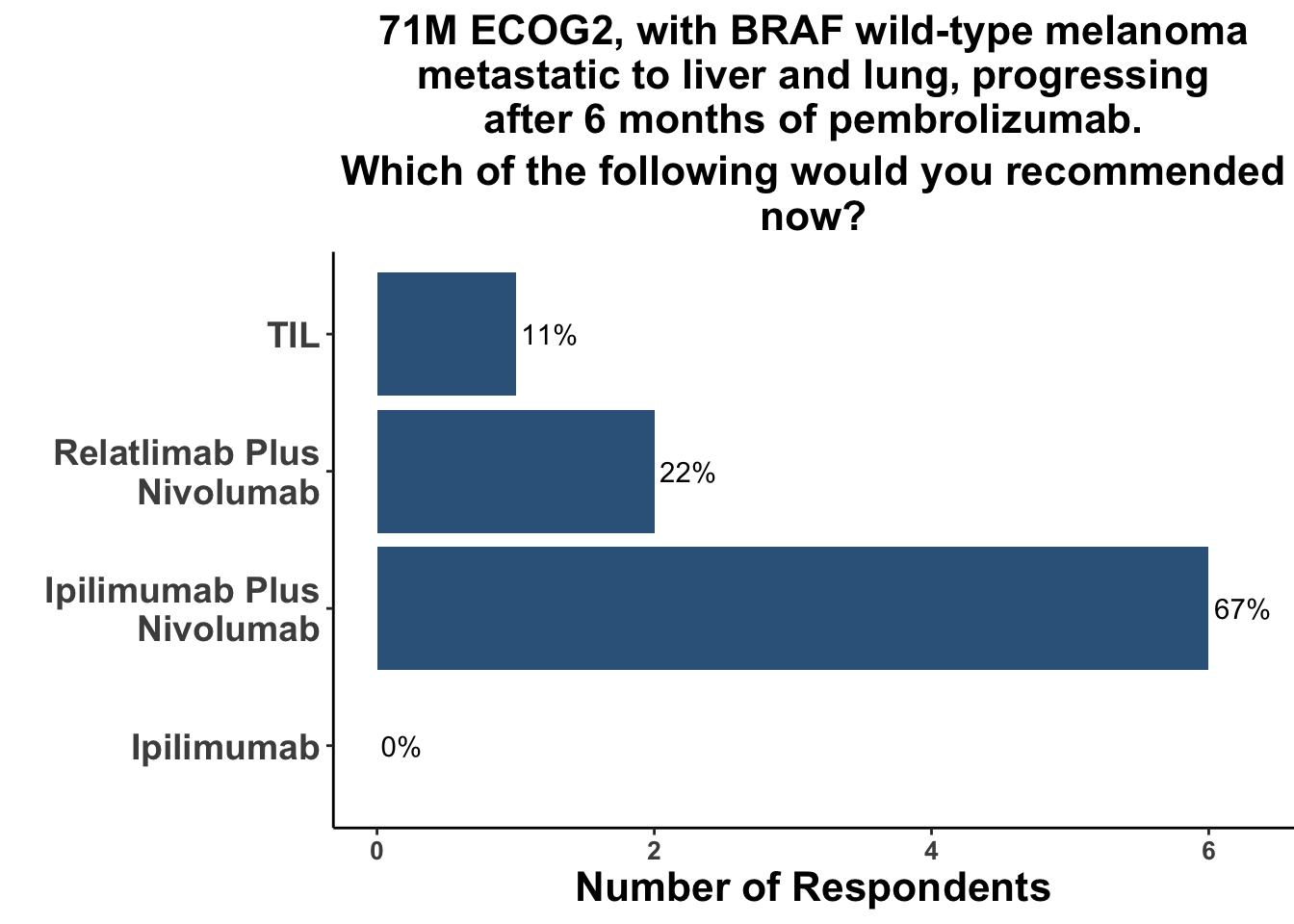
Improving outcomes for patients with ICI-refractory disease is a critical need. The treatment landscape is evolving and clinicians currently only have a few options to choose from when patients progress on first-line anti-PD-1 monotherapy. Commercially-available options include monotherapy ipilimumab, dual ICB with ipilimumab/nivolumab or ipilimumab/relatlimab and combination targeted therapies for patients with actionable BRAF V600 mutations. When provided with a clinical vignette of ICI-refractory wild-type melanoma, the vast majority of the diverse group of COIG attendees at the January 9th journal club that treat melanoma (Figure 5) responded that they would have selected combination ipilimumab/nivolumab (Figure 6). Given the patient’s ECOG status of 2, one respondent replied that they have recommended combination CTLA-4/LAG-3 in this case. None of the practioners would have recommended monotherapy ipilimumab.
Figure 5. Journal club attendees
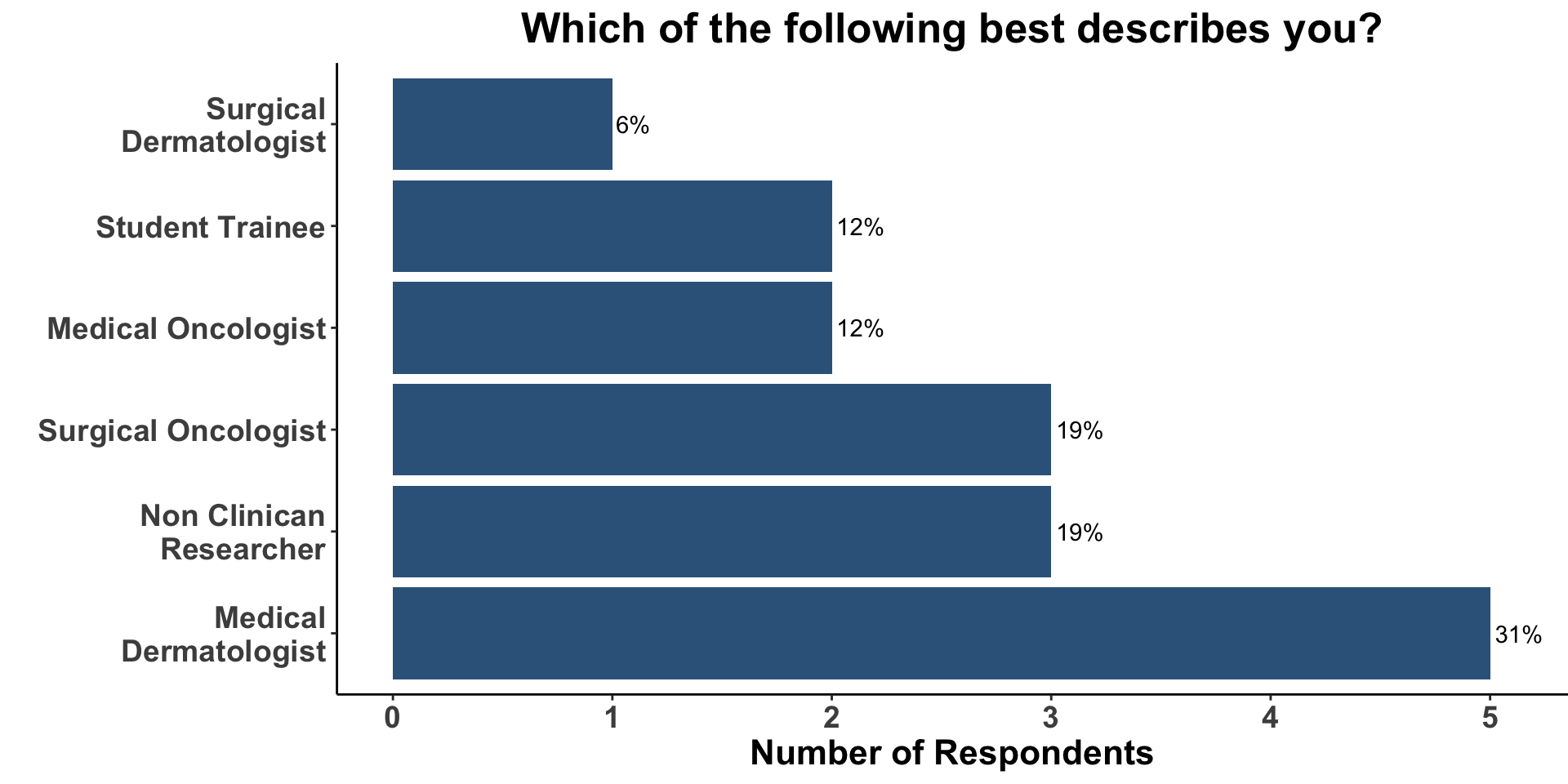
Figure 6. Management strategies of ICI-refractory melanoma
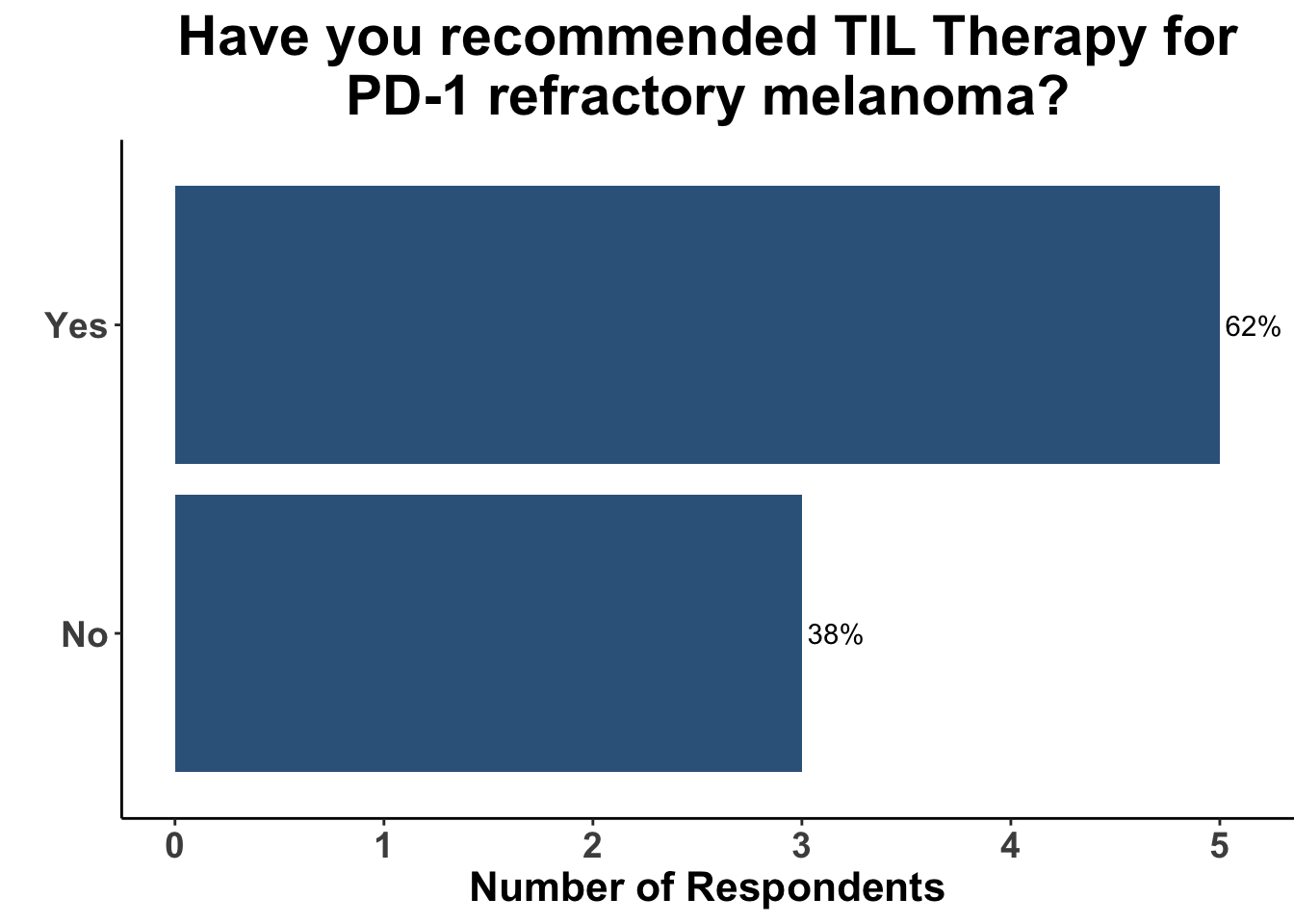
Attendees recognized that while dual ICB and combination oncogene-targeted therapies can produce responses in the second-line and beyond, meaningful clinical benefit is limited to a fraction of patients. For many years, TIL therapy has produced intriguing results in small, non-comparative investigations. Given the lack of commercial approval, TIL therapy has not been widely adopted. However, the majority of melanoma clinicians at the January 9th COIG JC have recommended TIL therapy previously as part of their practice (Figure 7). Some participants also recognized the importance of this paper as it is one of very few prospective, randomized trials of TIL therapy. While this is, in part, due to the challenges in identifying an appropriate control group, the data reported did identify a significant improvement in cinical outcome and a high ORR of 49% in a refractory melanoma population.
Figure 7. Experience with TIL therapy
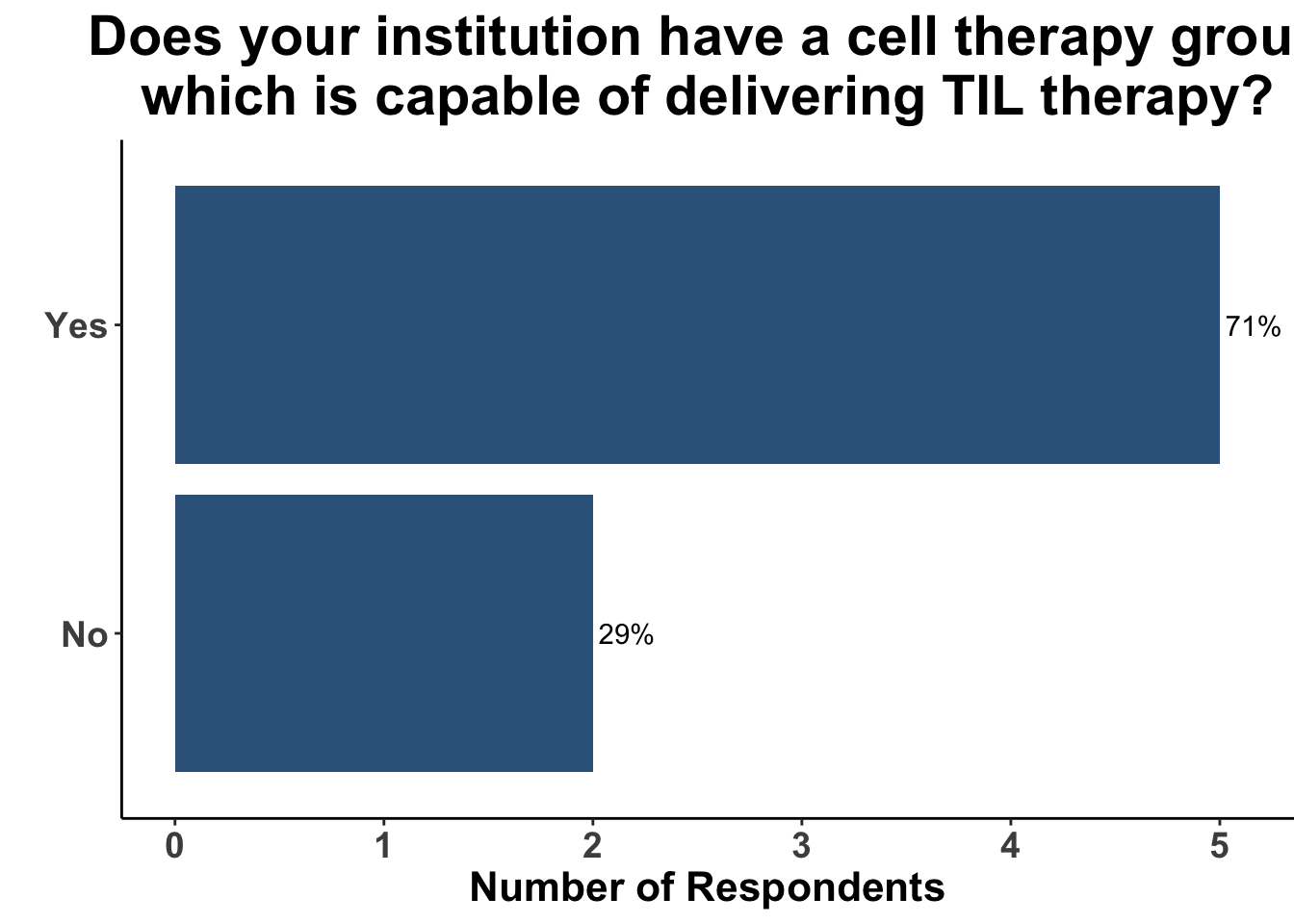
Furthermore, most were affiliates at institutions with a cell therapy group capable of delivery TIL therapy (Figure 8).
Figure 8. Cell therapy capabilities
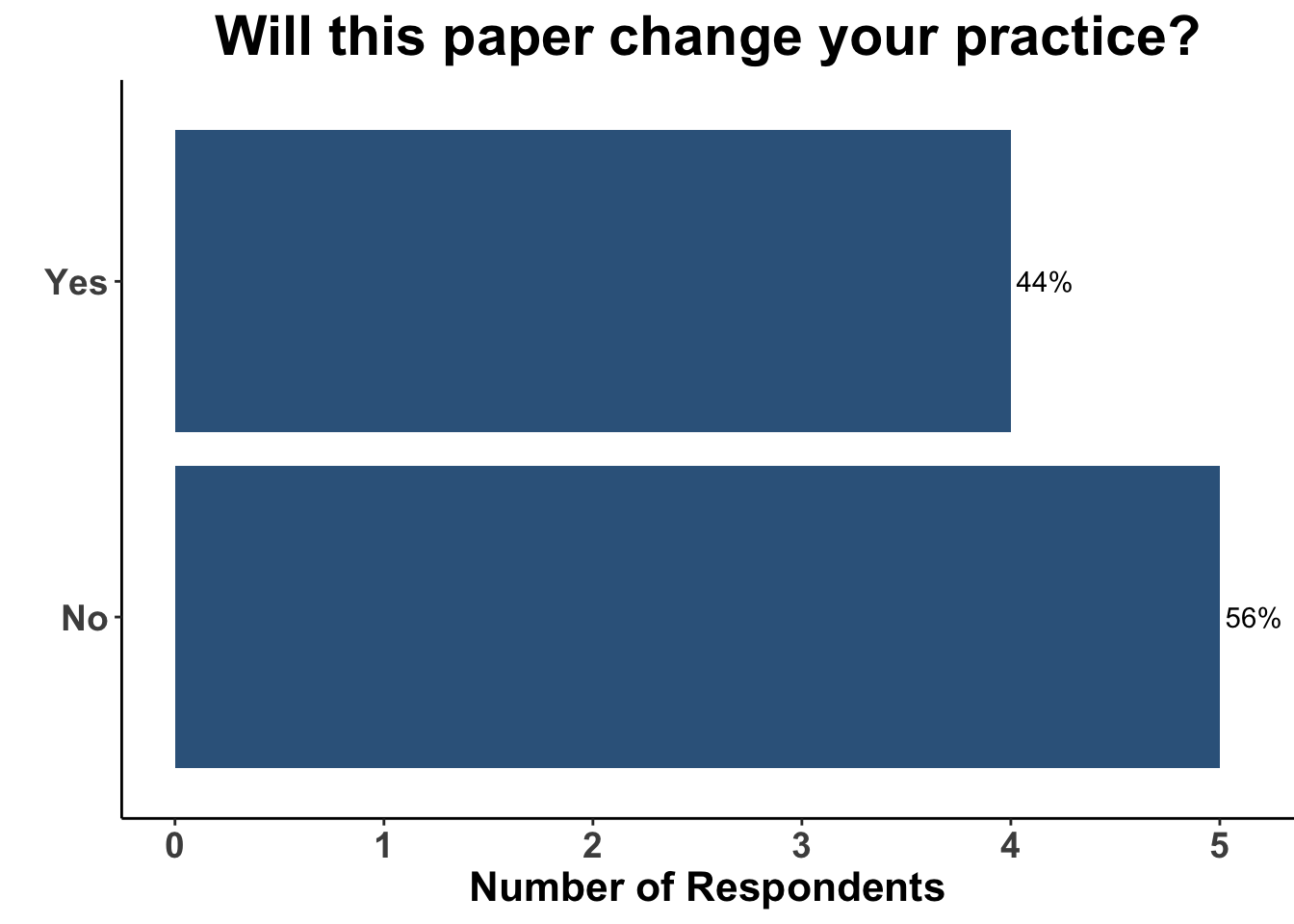
Thus, the results from Rohaan et al. were of a considerable interest. TIL therapy was associated with a clinically meaningful 50% reduction in the hazard for progression or death compared with monotherapy ipilimumab. Despite the majority of patients being treated previously with immunotherapy, nearly one-half of the patients experienced a response to TIL therapy. Importantly, responses were durable in the majority of patients that experienced an initial response. These data corroborate the findings in C-144-01, in which 15-20% of the heavily pre-treated cohort experienced durable responses following administration of lifileucel (Sarnaik et al. 2021). Taken collectively, TIL therapy is likely to become a standard option in the field. Indeed, Iovance, the sponsor of C-144-01, is expecting the rolling Biologics Licences Application (BLA) submission of lifileucel to be completed in the first half of 2023. Interestingly, while the attendees verbalized that the study by Rohaan et al. was a landmark investigation, less than half replied that it would change their practice (Figure 9).
Figure 9. Practice changing nature of the study
Indeed, when presented with the same case of refractory advanced melanoma, but given the option of having TIL therapy available, only 1/9 clinicians responded that they would recommend TIL therapy (Figure 10).
Figure 10. Case one revisted
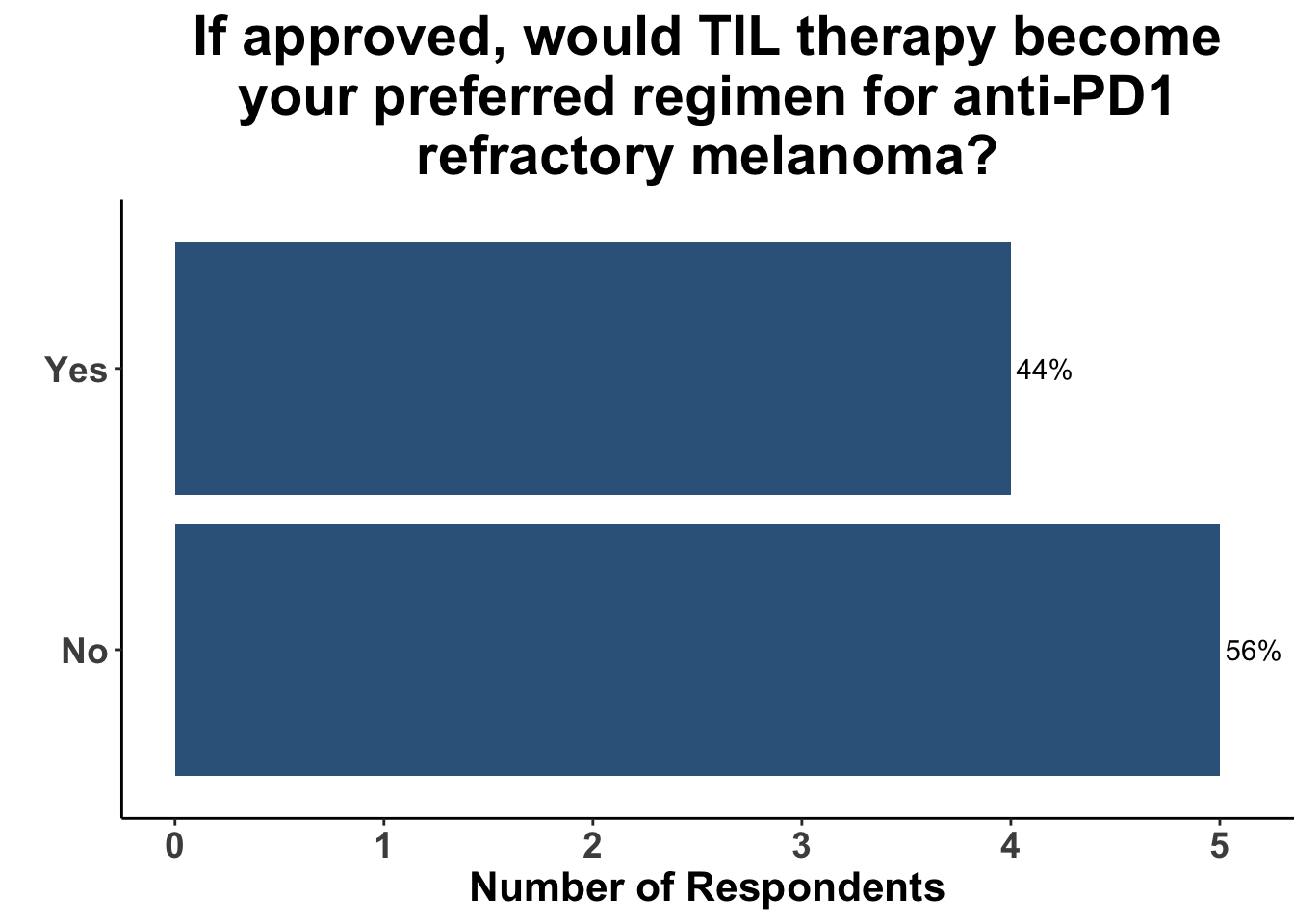
Only a minority of respondents replied that if approved, TIL therapy would become their preferred treatment strategy for PD-1 refractory melanoma (Figure 11). Toxicity and logistics of use were both discussed as considerations when selecting patients that might benefit from TIL therapy.
Figure 11. Implementation of TIL therapy
Despite the promise of TIL therapy, there are several challenges with its adoption and implementation. Most notably are the risks associate with its use. Grade 3 or higher treatment related adverse event (TRAEs) were nearly universal in both C-144-01 and the study by Rohaan et al. Granted, the vast majority were expected from the lymphodepleting agents used as part of the conditioning regimen, were transient and manageable. Nevertheless, 86% experienced the potentially life-threatening complication of febrile neutropenia and 10% of patients required transfer to the intensive care unit. When compared to the other treatment options for refractory disease, TIL therapy appears to offer a trade off of enhanced efficacy at the expense of increased toxicity (Figure 12).
Another consideration and potential barrier to TIL therapy are the logistics required for preparation. Adequate and accessible tumor tissue is needed, as is several weeks for cultivation and expansion of donor cells. Therefore, TILs may be less appropirate for patients with hard-to-access metastases and/or rapidly progressing disease. Thus, the use of TIL therapy is likely to be individualized and utilized in centers with experienced practioners. Nevertheless, the studies by Sarnaik et al. and Rohaan et al. reported a higher rate of TIL generation after harvesting suggesting improved technical capabilities to generate TIL are now available. In summary, these reports represent important contributions to the field and will likely lead to clinicians having additional options for their patients in the near future.
Materials and Methods
This Perspectives on the Science piece was published using Quarto®. The survey was conducted using REDCap® (Harris et al. 2009). The figures depicting the survey data were created using R (version 4.0.0) and the tidyverse suite of packages (Wickham et al. 2019), including ggplot2 (Wickham 2016). The figure depicting FDA approved therapies in melanoma was created using the skincancerRx package (Miller and Shalhout 2022).
References
Andersen, Rikke, Marco Donia, Eva Ellebaek, Troels Holz Borch, Per Kongsted, Trine Zeeberg Iversen, Lisbet Rosenkrantz Hölmich, et al. 2016. “Long-Lasting Complete Responses in Patients with Metastatic Melanoma After Adoptive Cell Therapy with Tumor-Infiltrating Lymphocytes and an Attenuated IL2 Regimen.” Clinical Cancer Research 22 (15): 3734–45. https://doi.org/10.1158/1078-0432.ccr-15-1879.
Atkins, Michael B., Sandra J. Lee, Bartosz Chmielowski, Ahmad A. Tarhini, Gary I. Cohen, Thach-Giao Truong, Helen H. Moon, et al. 2023. “Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients With Advanced BRAF-Mutant Melanoma: The DREAMseq TrialECOG-ACRIN EA6134.” Journal of Clinical Oncology 41 (2): 186–97. https://doi.org/10.1200/jco.22.01763.
Berg, Joost H van den, Bianca Heemskerk, Nienke van Rooij, Raquel Gomez-Eerland, Samira Michels, Maaike van Zon, Renate de Boer, et al. 2020. “Tumor Infiltrating Lymphocytes (TIL) Therapy in Metastatic Melanoma: Boosting of Neoantigen-Specific T Cell Reactivity and Long-Term Follow-up.” Journal for ImmunoTherapy of Cancer 8 (2): e000848. https://doi.org/10.1136/jitc-2020-000848.
Besser, Michal J., Ronnie Shapira-Frommer, Avraham J. Treves, Dov Zippel, Orit Itzhaki, Liat Hershkovitz, Daphna Levy, et al. 2010. “Clinical Responses in a Phase II Study Using Adoptive Transfer of Short-Term Cultured Tumor Infiltration Lymphocytes in Metastatic Melanoma Patients.” Clinical Cancer Research 16 (9): 2646–55. https://doi.org/10.1158/1078-0432.ccr-10-0041.
Dudley, Mark E., James C. Yang, Richard Sherry, Marybeth S. Hughes, Richard Royal, Udai Kammula, Paul F. Robbins, et al. 2008. “Adoptive Cell Therapy for Patients With Metastatic Melanoma: Evaluation of Intensive Myeloablative Chemoradiation Preparative Regimens.” Journal of Clinical Oncology 26 (32): 5233–39. https://doi.org/10.1200/jco.2008.16.5449.
Dudley, Mark, Wunderlich John, James Yang, Douglas J Patrick Hwu Schwartzentruber, Suzanne L Topalian, and Susan F Leitman Richard M Sherry Francesco M Marincola. 2022. “A Phase i Study of Nonmyeloablative Chemotherapy and Adoptive Transfer of Autologous Tumor Antigen-Specific t Lymphocytes in Patients with Metastatic Melanoma.” Journal of Immunotherapy. https://doi.org/10.1097/01.CJI.0000016820.36510.89.
Dummer, Reinhard, Paolo A Ascierto, Helen J Gogas, Ana Arance, Mario Mandala, Gabriella Liszkay, Claus Garbe, et al. 2018. “Encorafenib Plus Binimetinib Versus Vemurafenib or Encorafenib in Patients with BRAF -Mutant Melanoma (COLUMBUS): A Multicentre, Open-Label, Randomised Phase 3 Trial.” The Lancet Oncology 19 (5): 603–15. https://doi.org/10.1016/s1470-2045(18)30142-6.
Ellebaek, Eva, Trine Zeeberg Iversen, Niels Junker, Marco Donia, Lotte Engell-Noerregaard, Özcan Met, Lisbet Rosenkrantz Hölmich, et al. 2012. “Adoptive Cell Therapy with Autologous Tumor Infiltrating Lymphocytes and Low-Dose Interleukin-2 in Metastatic Melanoma Patients.” Journal of Translational Medicine 10 (1). https://doi.org/10.1186/1479-5876-10-169.
Hamid, O., C. Robert, A. Daud, F. S. Hodi, W. J. Hwu, R. Kefford, J. D. Wolchok, et al. 2019. “Five-Year Survival Outcomes for Patients with Advanced Melanoma Treated with Pembrolizumab in KEYNOTE-001.” Annals of Oncology 30 (4): 582–88. https://doi.org/10.1093/annonc/mdz011.
Harris, Paul A., Robert Taylor, Robert Thielke, Jonathon Payne, Nathaniel Gonzalez, and Jose G. Conde. 2009. “Research Electronic Data Capture (REDCap)A Metadata-Driven Methodology and Workflow Process for Providing Translational Research Informatics Support.” Journal of Biomedical Informatics 42 (2): 377–81. https://doi.org/10.1016/j.jbi.2008.08.010.
Long, Georgina V., F. Stephen Hodi, Evan J. Lipson, Dirk Schadendorf, Paolo Antonio Ascierto, Luis Matamala, Pamela Salman, et al. 2022. “Relatlimab and Nivolumab Versus Nivolumab in Previously Untreated Metastatic or Unresectable Melanoma: Overall Survival and Response Rates from RELATIVITY-047 (CA224-047).” Journal of Clinical Oncology 40 (36_suppl): 360385–85. https://doi.org/10.1200/jco.2022.40.36_suppl.360385.
Miller, David, and Sophia Shalhout. 2022. skincancerRx: Generates Visualizations for Data Related to FDA Approvals in Skin Cancer.
Petrella, Teresa M., Caroline Robert, Erika Richtig, Wilson H. Miller, Giuseppe V. Masucci, Euan Walpole, Celeste Lebbe, et al. 2017. “Patient-Reported Outcomes in KEYNOTE-006, a Randomised Study of Pembrolizumab Versus Ipilimumab in Patients with Advanced Melanoma.” European Journal of Cancer 86 (November): 115–24. https://doi.org/10.1016/j.ejca.2017.08.032.
Pilon-Thomas, Shari, Lisa Kuhn, Sabine Ellwanger, William Janssen, Erica Royster, Suroosh Marzban, Ragini Kudchadkar, et al. 2012. “Efficacy of Adoptive Cell Transfer of Tumor-Infiltrating Lymphocytes After Lymphopenia Induction for Metastatic Melanoma.” Journal of Immunotherapy 35 (8): 615–20. https://doi.org/10.1097/cji.0b013e31826e8f5f.
Pires da Silva, Ines, Tasnia Ahmed, Irene L M Reijers, Alison M Weppler, Allison Betof Warner, James Randall Patrinely, Patricio Serra-Bellver, et al. 2021. “Ipilimumab Alone or Ipilimumab Plus Anti-PD-1 Therapy in Patients with Metastatic Melanoma Resistant to Anti-PD-(L)1 Monotherapy: A Multicentre, Retrospective, Cohort Study.” The Lancet Oncology 22 (6): 836–47. https://doi.org/10.1016/s1470-2045(21)00097-8.
Robert, Caroline, Jean J. Grob, Daniil Stroyakovskiy, Boguslawa Karaszewska, Axel Hauschild, Evgeny Levchenko, Vanna Chiarion Sileni, et al. 2019. “Five-Year Outcomes with Dabrafenib Plus Trametinib in Metastatic Melanoma.” New England Journal of Medicine 381 (7): 626–36. https://doi.org/10.1056/nejmoa1904059.
Robert, Caroline, Antoni Ribas, Jacob Schachter, Ana Arance, Jean-Jacques Grob, Laurent Mortier, Adil Daud, et al. 2019. “Pembrolizumab Versus Ipilimumab in Advanced Melanoma (KEYNOTE-006): Post-Hoc 5-Year Results from an Open-Label, Multicentre, Randomised, Controlled, Phase 3 Study.” The Lancet Oncology 20 (9): 1239–51. https://doi.org/10.1016/s1470-2045(19)30388-2.
Robert, Caroline, Jacob Schachter, Georgina V. Long, Ana Arance, Jean Jacques Grob, Laurent Mortier, Adil Daud, et al. 2015. “Pembrolizumab Versus Ipilimumab in Advanced Melanoma.” New England Journal of Medicine 372 (26): 2521–32. https://doi.org/10.1056/nejmoa1503093.
Rohaan, Maartje W., Troels H. Borch, Joost H. van den Berg, Özcan Met, Rob Kessels, Marnix H. Geukes Foppen, Joachim Stoltenborg Granhøj, et al. 2022. “Tumor-Infiltrating Lymphocyte Therapy or Ipilimumab in Advanced Melanoma.” New England Journal of Medicine 387 (23): 2113–25. https://doi.org/10.1056/nejmoa2210233.
Rosenberg, S. A., J. R. Yannelli, J. C. Yang, S. L. Topalian, D. J. Schwartzentruber, J. S. Weber, D. R. Parkinson, C. A. Seipp, J. H. Einhorn, and D. E. White. 1994. “Treatment of Patients With Metastatic Melanoma With Autologous Tumor-Infiltrating Lymphocytes and Interleukin 2.” JNCI Journal of the National Cancer Institute 86 (15): 1159–66. https://doi.org/10.1093/jnci/86.15.1159.
Rosenberg, Steven A., James C. Yang, Richard M. Sherry, Udai S. Kammula, Marybeth S. Hughes, Giao Q. Phan, Deborah E. Citrin, et al. 2011. “Durable Complete Responses in Heavily Pretreated Patients with Metastatic Melanoma Using T-Cell Transfer Immunotherapy.” Clinical Cancer Research 17 (13): 4550–57. https://doi.org/10.1158/1078-0432.ccr-11-0116.
Sarnaik, Amod A., Omid Hamid, Nikhil I. Khushalani, Karl D. Lewis, Theresa Medina, Harriet M. Kluger, Sajeve S. Thomas, et al. 2021. “Lifileucel, a Tumor-Infiltrating Lymphocyte Therapy, in Metastatic Melanoma.” Journal of Clinical Oncology 39 (24): 2656–66. https://doi.org/10.1200/jco.21.00612.
Schachter, Jacob, Antoni Ribas, Georgina V Long, Ana Arance, Jean-Jacques Grob, Laurent Mortier, Adil Daud, et al. 2017. “Pembrolizumab Versus Ipilimumab for Advanced Melanoma: Final Overall Survival Results of a Multicentre, Randomised, Open-Label Phase 3 Study (KEYNOTE-006).” The Lancet 390 (10105): 1853–62. https://doi.org/10.1016/s0140-6736(17)31601-x.
Tawbi, Hussein A., Dirk Schadendorf, Evan J. Lipson, Paolo A. Ascierto, Luis Matamala, Erika Castillo Gutiérrez, Piotr Rutkowski, et al. 2022. “Relatlimab and Nivolumab Versus Nivolumab in Untreated Advanced Melanoma.” New England Journal of Medicine 386 (1): 24–34. https://doi.org/10.1056/nejmoa2109970.
Wickham, Hadley. 2016. Ggplot2: Elegant Graphics for Data Analysis. Springer-Verlag New York. https://ggplot2.tidyverse.org.
Wickham, Hadley, Mara Averick, Jennifer Bryan, Winston Chang, Lucy D’Agostino McGowan, Romain François, Garrett Grolemund, et al. 2019. “Welcome to the Tidyverse” 4: 1686. https://doi.org/10.21105/joss.01686.
Wolchok, Jedd D., Vanna Chiarion-Sileni, Rene Gonzalez, Piotr Rutkowski, Jean-Jacques Grob, C. Lance Cowey, Christopher D. Lao, et al. 2017. “Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma.” New England Journal of Medicine 377 (14): 1345–56. https://doi.org/10.1056/nejmoa1709684.
Appendix
Disclosures
DMM reports grants and personal fees from Regeneron, grants from Kartos Therapeutics, grants from NeoImmuneTech, personal fees from Checkpoint Therapeutics, personal fees from Pfizer, personal fees from Merck Sharpe & Dome, personal fees from EMD Serono, grants from Project DataSphere, personal fees from Sanofi Genzyme, personal fees from Castle Biosciences, personal fees from Avstera, outside the submitted work. EYK and SZS report no competing interests. HLK is an employee of Ankyra Therapeutics and serves on advisory boards for Marengo Therapeutics, Castle Bioscience, Virogin and MidaTech Pharma. VAP reports consulting honorarium from Regeneron, PhD Biosciences, Jounce Therapuetics, Almirall, and Castle Biosciences, and stock options from Avstera and Lazarus AI.
Disclaimer
This site represents our opinions only. See our full Disclaimer
Reuse
This work is licensed under a creative commons BY-NC-ND license

Citation
BibTeX citation:
@article{y_kim2023,
author = {Y Kim, Emily and Z. Shalhout, Sophia and L. Kaufman, Howard
and S. Emerick, Kevin and A. Patel, Vishal and Garmen, Khalid and
Brownell, Isaac and M. Miller, David},
editor = {M. Miller, David},
publisher = {Cutaneous Oncology Interest Group},
title = {Tumor-Infiltrating {Lymphocyte} {Therapy} for {Advanced}
{Melanoma:} {Ready} for {Prime} {Time?}},
journal = {Journal of Cutaneous Oncology},
volume = {1},
number = {1},
date = {2023-01-09},
url = {https://journalofcutaneousoncology.io/perspectives/til_therapy_for_advanced_melanoma/},
doi = {10.59449/joco.2023.01.09},
issn = {2837-1933},
langid = {en}
}
For attribution, please cite this work as:
Y Kim, Emily, Sophia Z. Shalhout, Howard L. Kaufman, Kevin S. Emerick,
Vishal A. Patel, Khalid Garmen, Isaac Brownell, and David M. Miller.
2023. “Tumor-Infiltrating Lymphocyte Therapy for Advanced
Melanoma: Ready for Prime Time?” Edited by David M. Miller.
Journal of Cutaneous Oncology 1 (1). https://doi.org/10.59449/joco.2023.01.09.