Clinical Utility of Cell-free DNA Liquid Biopsies in Merkel Cell Carcinoma
Article and Authorship Details
Journal: Dermatology Online Journal (postprint). Accepted August 20, 2021. © The Regents of the University of California, Davis campus. Please see the publisher’s version on the Dermatolgoy Online Journal website
Authors: Sophia Z. Shalhout, PhD1,2, Kevin S. Emerick,3, MD, Howard L. Kaufman, MD, PhD,4 and David Michael Miller, MD, PhD1,2
Affiliations:
1 Department of Medicine, Division of Hematology/Oncology, Massachusetts General Hospital, Harvard Medical School, Bartlett Hall, Room 132, 15 Parkman St, Boston, MA 02114, USA
2 Department of Dermatology, Massachusetts General Hospital, Harvard Medical School, Bartlett Hall, Room 132, 15 Parkman St, Boston, MA 02114, USA
3 Department of Otolaryngology, Massachusetts Eye and Ear Infirmary, Harvard Medical School, Boston, MA, USA
4 Department of Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA
Keywords: Liquid Biopsy, advanced merkel cell carcinoma, cell-free DNA, MCC, circulating free tumor DNA, ctDNA
Funding sources: This work was supported by Project Data Sphere, the American Skin Association, and ECOG-ACRIN.
Potential conflicts of interest: The authors declare the following potential conflicts. DMM has received honoraria for participating on advisory boards for Checkpoint Therapeutics, EMD Serono, Pfizer, Merck, Regeneron and Sanofi Genzyme. This article reflects the views of the authors only.
Abbreviations: AJCC: American Joint Committee on Cancer; CTCs: circulating tumor cells; cfDNA: cell-free DNA; CNA: Copy Number Alterations; FDA: US Food and Drug Administration; IHC: Immunohistochemistry; indels: insertions/deletions; IRB: Institutional Review Board; LiqBx: Liquid Biopsy; MCC: Merkel cell carcinoma; MCPyV: Merkel Cell Polyoma Virus; MS: Multiple Sclerosis; ST: Supplemental Table; NHL: Non-Hodgkin lymphoma; NGS: Next Generation Sequencing; RA: Rheumatoid Arthritis; SNV: Single Nucleotide Variants; TMB: tumor mutational burden; TTE: transthoracic echocardiogram
To the Editor:
Merkel Cell Carcinoma (MCC) is a rare and aggressive neuroendocrine cutaneous malignancy characterized by the variable presence of Merkel cell polyoma virus (MCPyV), programmed cell death ligand-1 (PD-L1) expression and variable mutation burden status. These varying molecular features have made development of standardized prognostic and predictive biomarkers challenging. MCC patients may be screened for viral oncoprotein antibodies since serum titer levels in MCPyV-positive patients reflect MCC tumor burden and are a strong marker for recurrence[1-2]. However, this assay may not be reliable in immunosuppressed patients and those treated with immunotherapy. Furthermore, it is not useful for monitoring ~50% of MCC patients that are MCPyV-negative. Thus, additional non-invasive modalities are needed for prognosis and monitoring disease-status in all MCC patients, including MCPyV-negative patients.
Liquid biopsy, which allows for the sequential analysis of circulating tumor cells (CTCs) or cell-free DNA (cfDNA) in blood samples, has recently emerged as a potential non-invasive approach for surveillance, prognosis, and guidance for therapeutic options in several cancers. Few previous studies evaluated the CellSearch™ liquid biopsy system which isolates epithelial cell adhesion molecule (EpCAM) positive CTCs in MCC. CTCs were found associated with MCC disease burden and shorter overall survival [3-5]. While promising, further studies are required to determine the potential use of liquid biopsy in managing MCC patients. The objective of this study was to assess the clinical utility of cell-free DNA (cfDNA) next-generation sequencing (NGS) in MCC.
We performed an institutional review board-approved study of MCC patients at Mass General Brigham who underwent cfDNA-sequencing using an expanded cancer-associated gene panel of the US Food and Drug Administration (FDA)-approved Guardant360® platform under physician-discretion standard-of-care (N=16). Fifteen of these patients also had matched genotyping of primary MCC tumor tissue using targeted next generation sequencing with institutional SNaPshot-NGS assay. Tumor burden at the time of blood collection was evaluated using Response Evaluation Criteria in Solid Tumors version 1.1 (RECISTv1.1). Pearson’s correlation was used to assess association between tumor burden and the highest allelic frequency detected in cfDNA analysis. Fisher’s exact test were used to model associations between cfDNA detection and active MCC disease. Patients with indeterminant status as the time of blood collection were included in the analysis based on the unequivocal true disease status (N=3 no evidence of disease, N=1 regional/distant disease). Given that this is an exploratory analysis of a limited sample size from a single institution with no regulatory implications, dichotomous significance testing was not performed, and p-values were exploratory only. Bonferroni corrections were not applied. R software version 4.0 was used to analyze data from the REDCap database “Merkel Cell Carcinoma Patient Registry” using the REDCap application programming interface and R packages: REDCapR, ggpubr and tidyverse.
Twelve (75%) patients had regional/distant metastasis, and three (19%) patients had no clinical or radiographic evidence of disease at the time of blood collection (Table 1).
Table 1: Patient Characteristics
| Patient Characteristics | N = 16 |
|---|---|
| Age | |
| Median age, years (range) | 77 (56-95) |
| Race | |
| White | 16 (100) |
| Sex | |
| Male | 15 (94) |
| Female | 1 (6) |
| Merkel Cell Polyoma Virus (MCPyV) Titer Status | |
| Positive^a^ | 6 (38) |
| Negative | 10 (62) |
| Site of MCC | |
| Primary Cutaneous | 13 (81) |
| Face | 6 (38) |
| Extremities | 4 (25) |
| Trunk | 3 (19) |
| Unknown Primary | 3 (19) |
| Inguinal Lymph Nodes | 2 (13) |
| Parotid Gland | 1 (6) |
| Primary Tissue Genotyped | 15 (94) |
| Lymphovascular Invasion | 7 (44) |
| Lymph Node Involvement | 14 (88) |
| Clinical Stage at Presentation (AJCC 8th Ed.) | |
| Stage I | 4 (25) |
| Stage IIA | 3 (18) |
| Stage III | 7 (44) |
| Stage IV | 2 (13) |
| Extent of MCC Disease at Time of Liquid Bx | |
| Local | 1 (6) |
| Regional and/or Distant Metastasis | 12 (75) |
| No evidence of disease^b^ | 3 (19) |
| History of Immunosuppresion | |
| No | 13 (81) |
| Yes | 3 (19) |
| HIV and Non-Hodgkin Lymphoma^c^ | 1 |
| Immunosuppressing Medical Therapy^d^ | 1 |
| Rheumatoid Arthritis^e^ | 1 |
| Note: | |
| Abbreviations: AJCC: American Joint Committee on Cancer; IHC: Immunohistochemistry; LiqBx: Liquid Biopsy; RA: Rheumatoid Arthritis; NHL: Non-Hodgkin Lymphoma; MCPyV: Merkel Cell Polyoma Virus; MS: Multiple Sclerosis; TMB: tumor mutational burden | |
| a One patient had MCPyV- positive status confirmed with only IHC of MCC tumor tissue and never received an MCPyV antibody serum titer level test. | |
| b Three patients with indeterminate disease at the time of liquid biopsy were confirmed eventually to have no evidence of MCC disease, in agreement with no cfDNA detection. One patient with indeterminate disease went on to have metastatic disease in agreement with high cfDNA and TMB-high results | |
| c Rituximab and anti-neoplastic chemotherapy for NHL | |
| d Longstanding history of Copaxone for demyelinating MS | |
| e Methotrexate and Prednisone for RA | |
Additional patient characteristics are summarized in Table 1. cfDNA detection was strongly associated with active MCC disease at the time of sample acquisition (p-value = 0.007). In MCPyV-negative patients with regional/distant disease, at least one matched genetic variant in cfDNA and primary MCC tissue was detected in all patients (7/7). cfDNA was detected in each MCPyV-positive patient with regional/distant disease (5/5). However, only low allelic frequency (<2%) mutations in ATM, NF1, TP53, NTRK, ARID1A, and MET were detected and did not match the mutations found in primary tissue; therefore, clonal hematopoiesis of indeterminate potential cannot be ruled out (Table 2). cfDNA was not detected in patients that had no evidence of disease (3/3) or only localized, sub-centimeter neuroendocrine carcinoma of the skin (1/1). MCC tumor burden significantly correlated with the highest cfDNA variant allele fraction (Pearson’s correlation=0.7, p-value=0.046) in the MCPyV-negative population. Only a moderate trend was observed in MCPyV-positive subjects (Pearson’s correlation=0.48, p-value=0.33), and was not statistically significant.
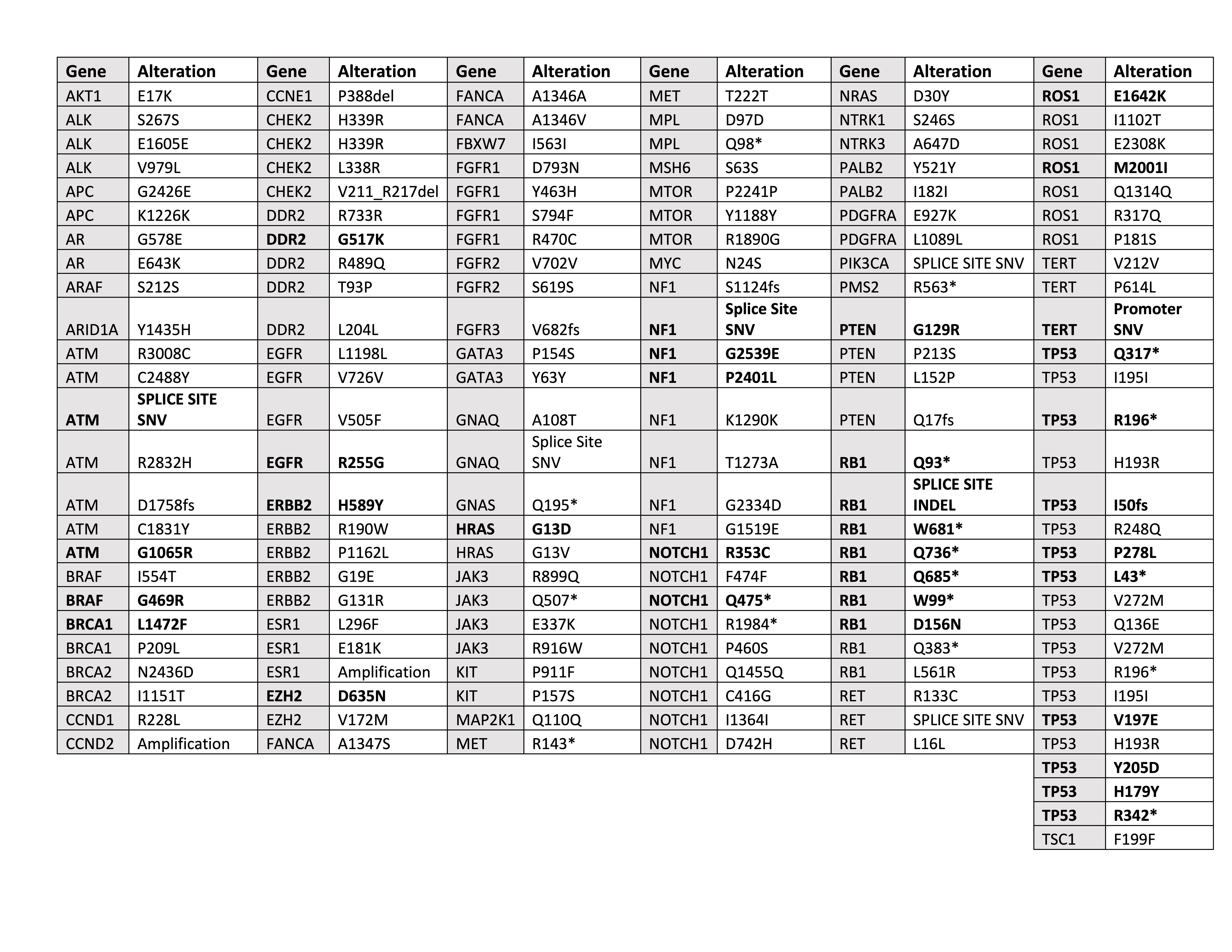 Table 2: Genetic Alterations detected in cfDNA analysis The mutations detected in cfDNA analysis with Guardant360 are listed below. The mutations/alterations that matched primary tissue mutations as detected with the SNaPshot-NGS assay are shown in bold. Note that primary genotyping covered a larger gene panel and in the case of low allelic fractions detected on cfDNA, clonal hematopoiesis of indeterminant potential cannot be ruled out as discussed.
Table 2: Genetic Alterations detected in cfDNA analysis The mutations detected in cfDNA analysis with Guardant360 are listed below. The mutations/alterations that matched primary tissue mutations as detected with the SNaPshot-NGS assay are shown in bold. Note that primary genotyping covered a larger gene panel and in the case of low allelic fractions detected on cfDNA, clonal hematopoiesis of indeterminant potential cannot be ruled out as discussed.
In summary, we utilized an FDA-approved commercially available liquid biopsy test to detect cfDNA in MCC and provide the first evaluation of cfDNA in the management of MCC patients. Although Guardant360® was reliable and effective in detecting MCC recurrence and minimal residual disease in MCPyV-negative patients, MCPyV-positive tumors may require liquid biopsy platforms with deeper sequencing and broader coverage due to limited mutations driving virus-positive cancers[6]. In addition, a patient-specific approach utilizing the individual’s primary tumor mutations to inform a personalized cfDNA gene panel may prove useful in detecting cfDNA since MCPyV-positive cancers are generally tumor mutation burden-low[7]. Furthermore, we acknowledge that further large-scale studies of cfDNA analysis with serial blood samples are warranted to evaluate its clinical utility. However, in rare disease such as MCC, the feasibility of appropriately powered prospective studies to thoroughly evaluate such technologies is limited. Therefore, single-institution case series can establish important proof-of-concept data to guide future studies, as well as early clinical adoption. In this single-institution case series, liquid biopsy proved clinically useful in the management of several cases and highlights potential scenarios where cfDNA analysis may be applied. For example, liquid biopsies have the potential to aid clinicians in the confirmation of metastatic disease in the setting of challenging-to-obtain visceral lesions. In one case in our series, a patient developed an atrial mass concerning for thrombus versus neoplasm. Cardiac imaging and cfDNA with concordant mutations found in the primary tumor supported metastatic disease (Figure 1).
Figure 1: Timeline of Patient Course A patient with Merkel Cell Carcinoma of unknown primary was effectively treated with radiotherapy and pembrolizumab but went on to develop an atrial mass concerning for thrombus versus neoplasm. Liquid biopsy revealed cfDNA with concordant mutations found in the primary tumor tissue which supported metastatic MCC. While eventually biopsied and confirmed via histologic examination, liquid biopsy was obtained several days prior and resulted ahead of the histological confirmation allowing for prompt radiotherapy planning.
MCC was subsequently confirmed via histologic examination; however, due to technical challenges of the heart biopsy, liquid biopsy was obtained several days prior and resulted ahead of the histological confirmation. Although tissue confirmation of metastatic disease is the standard of care, there are situations in which the risks of obtaining tissue are quite high. Thus, a high-fidelity liquid biomarker may be appropriate for clinical decision-making in certain scenarios. In addition to potentially functioning as a circulating surrogate for distant disease, liquid biopsies may be able to predict a well-known and particularly concerning subtype: the early rapid progressor. In these patients there is swift development of widespread metastatic disease during the interval from initial work up and management, to the first follow up scan at three months. These patients are particularly challenging to manage as the progression to extensive-stage disease and rapid clinical decline can limit evaluation for clinical trials and end-of-life planning. In our case series, cfDNA analysis detected high-allelic fraction-disease in one patient despite no definitive evidence of disease on computed tomography performed days earlier. Widespread osseous and hepatic lesions were detected on repeat imaging just 8 weeks later. The patient subsequently succumbed to MCC less than one month following those scans. Thus, a tool that can serve as both a hematologic biomarker of metastatic disease as well as a predictor of rapid progression has obvious potential implications. Although confirmatory studies are needed, these data suggest that liquid biopsies may have several clinical applications for patients with MCC.
References:
1. Paulson KG, Carter JJ, Johnson LG, Cahill KW, Iyer JG, Schrama D, Becker JC, Madeleine MM, Nghiem P, Galloway DA. Antibodies to merkel cell polyomavirus T antigen oncoproteins reflect tumor burden in merkel cell carcinoma patients. Cancer Res. 2010 Nov 1;70(21):8388-97. doi: 10.1158/0008-5472.CAN-10-2128. Epub 2010 Oct 19. PMID: 20959478; PMCID: PMC2970647.
2. Paulson KG, Lewis CW, Redman MW, Simonson WT, Lisberg A, Ritter D, Morishima C, Hutchinson K, Mudgistratova L, Blom A, Iyer J, Moshiri AS, Tarabadkar ES, Carter JJ, Bhatia S, Kawasumi M, Galloway DA, Wener MH, Nghiem P. Viral oncoprotein antibodies as a marker for recurrence of Merkel cell carcinoma: A prospective validation study. Cancer. 2017 Apr 15;123(8):1464-1474. doi: 10.1002/cncr.30475. Epub 2016 Dec 7. PMID: 27925665; PMCID: PMC5384867.
3. Blom, A.; Bhatia, S.; Pietromonaco, S.; Koehler, K.; Iyer, J.G.; Nagase, K.; Paulson, K.; Sabath, D.E.; Nghiem, P.Clinical utility of a circulating tumor cell assay in Merkel cell carcinoma.J. Am. Acad. Dermatol.2014,70,449–455.
4. Riethdorf, S.; Hildebrandt, L.; Heinzerling, L.; Heitzer, E.; Fischer, N.; Bergmann, S.; Mauermann, O.;Waldispuhl-Geigl, J.; Coith, C.; Schon, G.; et al. Detection and Characterization of Circulating Tumor Cells inPatients with Merkel Cell Carcinoma.Clin. Chem.2019.
5. Boyer, M.; Cayrefourcq, L.; Garima, F.; Foulongne, V.; Dereure, O.; Alix-Panabieres, C. Circulating Tumor Cell Detection and Polyomavirus Status in Merkel Cell Carcinoma.Sci. Rep.2020,10, 1612. 6. Harms KL, Zhao L, Johnson B, Wang X, Carskadon S, Palanisamy N, Rhodes DR, Mannan R, Vo JN, Choi JE, Chan MP, Fullen DR, Patel RM, Siddiqui J, Ma VT, Hrycaj S, McLean SA, Hughes TM, Bichakjian CK, Tomlins SA, Harms PW. Virus-positive Merkel Cell Carcinoma Is an Independent Prognostic Group with Distinct Predictive Biomarkers. Clin Cancer Res. 2021 May 1;27(9):2494-2504. doi: 10.1158/1078-0432.CCR-20-0864. Epub 2021 Feb 5. PMID: 33547200.
7. Reinert T, Henriksen TV, et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients with Stages I to III Colorectal Cancer. JAMA Oncol. 2019 Aug 1;5(8):1124-1131. doi: 10.1001/jamaoncol.2019.0528. Erratum in: JAMA Oncol. 2019 Jun 13;: PMID: 31070691; PMCID: PMC6512280.